
Research
- Understanding genetic susceptibility of multiple cancers
- Studying the causes of cancer though genomic techniques
- Early detection of cancer to reduce mortality and morbidity
- Building global capacity for cancer science
- Somatic cancer genomics and molecular characterization of tumours
- Understanding variations in cancer incidence and survival
GEM’s work can be subdivided into six more general themes. These six areas are the following:
Area 1. Understanding genetic susceptibility of multiple cancersThis area is a long-standing and core area of GEM’s research work. GEM will continue to build upon and expand its previous successful efforts in identifying cancer susceptibility genes and how they influence cancer susceptibility. The genetic studies focus primarily on cancer sites for which GEM has established a leading role in bringing together large case–control studies and patient series in collaboration with colleagues worldwide, including for lung cancer, head and neck cancers, kidney cancer, and lymphomas. Where feasible, these studies will be expanded into understudied populations, and development will continue for the inclusion of genetic risk scores into cancer prevention programmes.
Projects:- Lung cancer. Within the International Lung Cancer Case–Control Consortium (ILCCO), GEM is undertaking a very large genetic study of lung cancers, with the goal of using genetic profiles to assist in targeting of low-dose computed tomography (LDCT) screening for early detection of lung cancer.
- Lymphomas. GEM is carrying out the largest genetic studies of lymphomas within the International Lymphoma Epidemiology Consortium (InterLymph).
- Head and neck cancers. GEM is coordinating a large genetic study of head and neck cancers across Europe, North America, Asia, and Latin America.
- Nasopharyngeal cancer. GEM is undertaking genetic studies of this cancer type, which is particularly relevant to South-East Asia.
This area focuses on improving the understanding of cancer etiology using genomic and epidemiological techniques. A large part of this work will focus on the successful conclusion of the Mutographs project, due to be completed in 2023, in which whole-genome sequencing data have been generated on more than 4000 cancers across multiple cancer types, including oesophageal, renal, colorectal, pancreatic, bladder, gallbladder, and head and neck cancers.
GEM is also using observational and genetic techniques in tandem to infer causality of putative risk factors and to identify novel modifiable risk factors for cancer. These projects rely heavily on traditional epidemiological analyses conducted in large cohort studies, such as the European Prospective Investigation into Cancer and Nutrition (EPIC) and the UK Biobank, and are complemented by extensive use of Mendelian randomization techniques, which avoid many biases that affect traditional epidemiology by use of genetic proxies.
Area 3. Early detection of cancer to reduce mortality and morbidityGEM is conducting several ambitious projects that aim to improve early detection of cancer through the development and validation of biomarker tests using pre-diagnostic biological samples within large cohort studies. The lung cancer work focuses on the potential for proteomic biomarkers to improve the identification of preclinical lung cancer, and their implementation within population-based screening studies by low-dose computed tomography (LDCT). Similarly, the studies on early detection of human papillomavirus (HPV)-related cancers investigate the potential for protein biomarkers to complement HPV antibody tests, for which an extremely high sensitivity and specificity has already been demonstrated. GEM is also investigating the potential utility of studies that focus on detection of the HPV viral genome in circulating free DNA (cfDNA). Finally, GEM is studying the potential for the detection of TERT promoter mutations in urine as non-invasive biomarkers for the early detection of bladder cancer in multicentre case–control and prospective cohort studies.
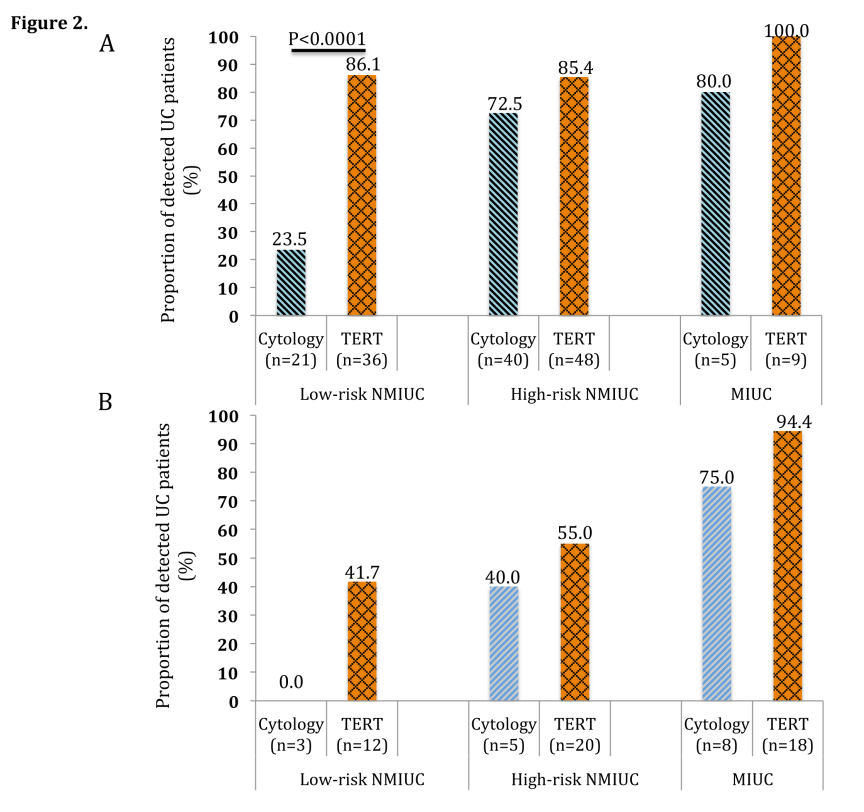
Figure 2.
Sensitivity of urine cytology and urinary TERT promoter mutations for detecting various risk categories of urothelial cancer (UC) in the DIAGURO case–control series in France. Tumours are categorized in three groups: low-risk non-muscle-invasive urothelial cancer (NMIUC) (pTa/pT1, low grade), high-risk NMIUC (pTa/pT1, high grade and any stage associated with carcinoma in situ), and muscle-invasive urothelial cancer (MIUC) (pT2, pT3, or pT4).
Reproduced with permission from Avogbe PH, Manel A, Vian E, Durand G, Forey N, Voegele C, et al. (2019). Urinary TERT promoter mutations as non-invasive biomarkers for the comprehensive detection of urothelial cancer. EBioMedicine. 44:431–8.
GEM scientists have a long history of bringing together and coordinating research consortia, and sharing research data within these collaborations is essential to advance the research agenda. Regulations aimed at protecting the privacy of research participants’ personal data have started to limit the rate at which GEM is able to share crucial research data across borders. Therefore, GEM has initiated a series of activities aimed at standardizing the processing of research data across IARC and within GEM, with a particular view to aligning the practices with the most relevant data protection regulations, including setting up a system that allows external collaborators to access various databases remotely without transferring individual-level data across borders and between institutes. The focus is on projects where GEM is actively leading consortium studies, initially with a focus on head and neck cancers, lymphomas, and lung cancer.
Area 5. Somatic cancer genomics and molecular characterization of tumoursGEM continues to expand upon its detailed genomic studies involving molecular characterization of a variety of cancer types, including renal cancers, neuroendocrine neoplasms, mesothelioma, and head and neck cancers. These studies will build upon the extensive investment made by IARC in high-performance computing, as well as the rich bioinformatic, computational biology, and genomics expertise within GEM.
Projects:- Integrated Omics analysis into Renal Cancer Incidence and Survival – the KidOmics project.
- Building the largest genomics resource of somatic and viral genetic changes involved in head and neck cancer onset and outcome in diverse populations.
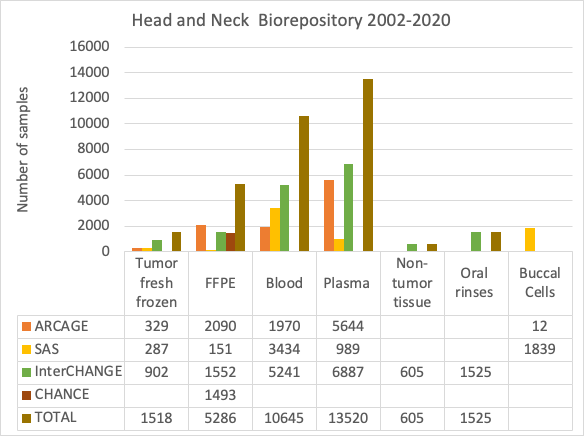
Figure 3.
Head and Neck Biorepository 2002–2020.
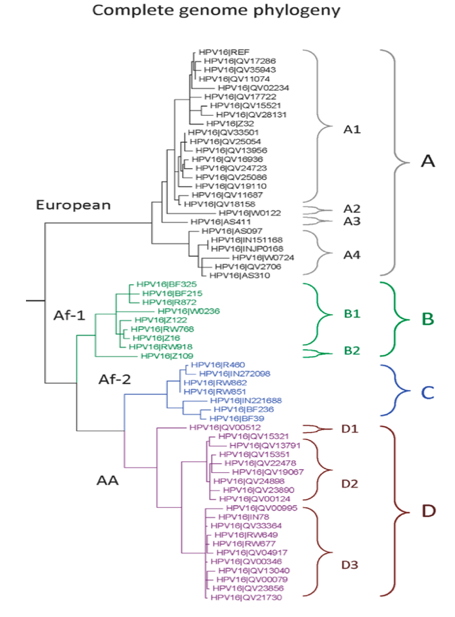
Figure 4.
Genome phylogeny of HPV16.
Reproduced with permission from Burk RD, Harari A, Chen Z. Human papillomavirus genome variants. Virology. 2013 Oct;445(1-2):232-43. doi: 10.1016/j.virol.2013.07.018. © Elsevier
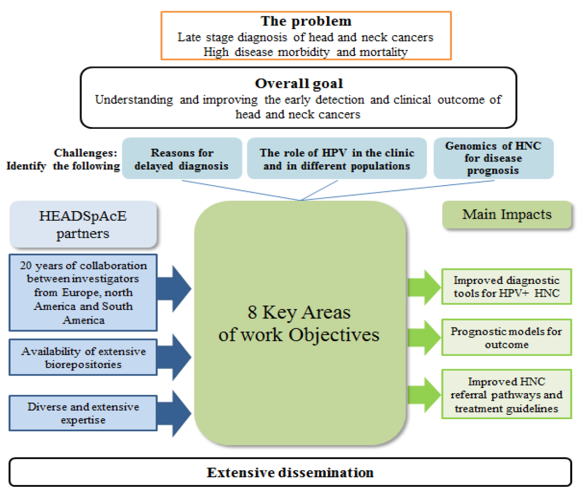
Figure 5.
Concept of the HEADSpAcE consortium.
- LungNENomics and panNENomics. Multidisciplinary and multi-omics molecular characterization of neuroendocrine neoplasms (NENs). NENs are ubiquitous diseases that may occur anywhere in the human body. GEM is currently focusing on lung neuroendocrine tumours (typical and atypical pulmonary carcinoids), with the aim of studying other body sites in the future.
- MESOMICS. French project of multi-omic characterization of malignant pleural mesothelioma, a rare, understudied cancer associated with exposure to asbestos. GEM is currently performing a full molecular characterization of malignant pleural mesothelioma types and subtypes through a multi-omics integrative analysis. The molecular data will be correlated with morphological (based on artificial intelligence), epidemiological, and clinical features.
- Investigating the heterogeneity of rare cancers through molecular maps. The aims of this project are to generate comprehensive molecular maps for lung NENs and malignant pleural mesothelioma, and to leverage these maps to study tumour heterogeneity using multi-regional sequencing at the single-cell resolution (Figure 6).
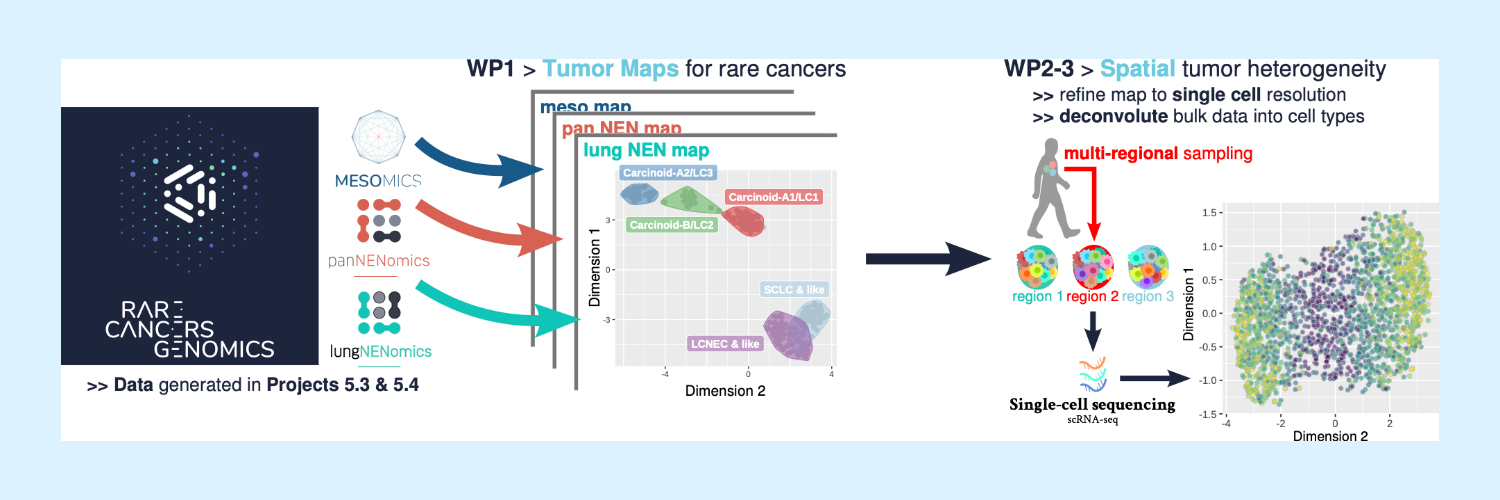
Figure 6.
Schematic overview of the “Investigating the heterogeneity of rare cancers through molecular maps” project.
- Unveiling the molecular pathways underlying tumour evolution through mechanistic and computational models. GEM aims to use the data and hypotheses generated in the lungNENomics and panNENomics projects and leverage the tumour maps to (i) mechanistically test hypotheses about the early events responsible for the transformation from normal neuroendocrine cell to neoplastic cell, and from low-grade to higher-grade neoplasms, and (ii) develop the statistical tools necessary to track the temporal changes occurring inside the tumour and the organoid across multiple -omics layers (Figure 7).
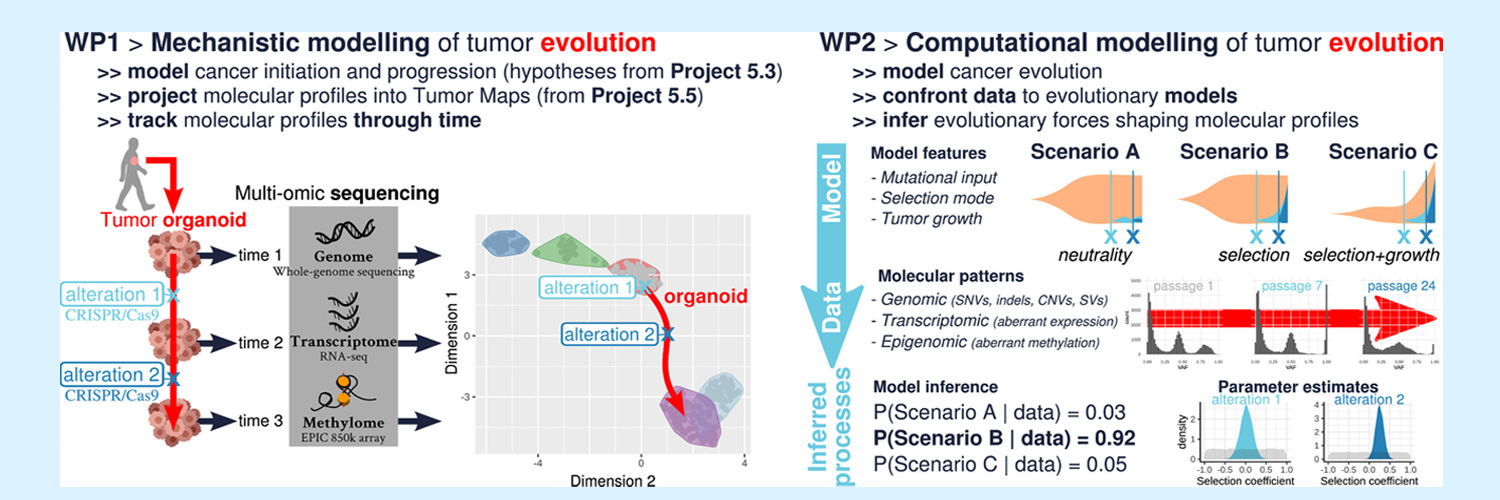
Figure 7.
Schematic of project design and methods. In WP1, the two-dimensional “tumour map” corresponds to the expression profiles of 238 NENs as summarized by the dimensionality reduction technique UMAP (data from Gabriel et al., GigaScience 2020). In WP2, “scenario” schematics represent the temporal dynamics of tumour clones sizes (beige: global tumour size, blue: subclones corresponding to the different alterations introduced), “molecular patterns” histograms correspond to the distribution of the variant allelic fraction of somatic alterations in the organoids at different time points (passages), and “parameter estimates” correspond to Bayesian probability distributions of the different model parameters given the observed data (grey: prior distributions, blue: posterior distributions).
This last area of GEM’s work includes a diverse group of projects that build upon various areas of GEM expertise to understand biological, environmental, and sociodemographic factors associated with differences in incidence and survival for major cancer sites, including cancers of the bladder, breast, head and neck, lung, and kidney. The studies use large biorepositories built from cohort and case series, with a specific focus on population diversity (inclusion of non-European and admixed populations) and integration of -omics data and clinical and epidemiological information.
Projects:- Understanding the causes of late diagnosis of head and neck cancers. How diagnostic delay is affected by additional factors, including psychosocial, financial, structural, and educational barriers, at various stages of the diagnostic and treatment process. GEM initiated studies on oral preneoplasia, with the goal of identifying those lesions that are liable to become cancerous.
- Clinical implementation of urinary TERT promoter mutations as biomarkers for monitoring minimal residual disease or recurrence or urothelial cancer (CLINITERT).
- GEM studies in the Islamic Republic of Iran contributed to the IARC Monographs programme’s classification of opium consumption as carcinogenic to humans (Group 1). GEM aims to further investigate a potential carcinogenic effect for opioids by initiating a new international study within a diverse group of population cohorts (OPICO).
- Genomic basis of breast cancer in understudied populations. GEM aims to identify the underlying causes of breast cancer in women in understudied populations, including the identification of etiological risk factors that could be potentially relevant for preventive interventions (BRiDGE).